
Podcast Ep 21: Galeazzi Fractures, Malnutrition, & More




Change your thoughts and you change your world.
-Norman Vincent Peale
Welcome back to Episode 21! We are all over the place this week, tackling topics from orthopedics to electrolyte abnormalities. Thanks to our listeners for the excellent feedback. Keep it coming to roshcast@roshreview.com. Let’s get started with a quick neurology rapid review from prior episodes!

- Treatment for a radial nerve palsy is supportive with a wrist splint, and the condition is typically self-limited.
- VP shunt obstruction occurs proximally more often than it occurs distally. Proximal VP shunt obstruction occurs due to choroid plexus obstruction or increased protein within the CSF. Distal VP shunt obstruction occurs due to abdominal pseudocyst formation, which typically presents with abdominal pain due to the large size of the cyst.
- Lyme disease is the most common cause of a bilateral Bell’s palsy. Remember that a peripheral facial nerve palsy can be distinguished from a central one by involvement of the forehead.
Now onto this week’s podcast
Question 1
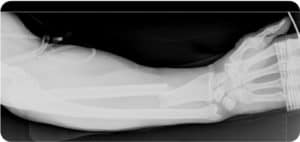
A patient presents to you as a transfer from an outside facility with the radiograph seen above. Which of the following exams will evaluate for the most commonly associated nerve injury in this type of fracture?
A. Ability to make a “thumbs up” sign
B. Ability to make an “OK” sign
C. Sensation to the index finger
D. Sensation to the little finger
Question 2
Which of the following is a common cause of hypomagnesemia?
A. Antacid use
B. Hypoparathyroidism
C. Hypothyroidism
D. Malnutrition
Question 3
A 24-year-old man is brought to the ED after sustaining a stab wound to the right side of his chest. He is diagnosed with a hemothorax and a 38-French chest tube is placed in the resuscitation room. Which of the following best predicts the need for urgent thoracotomy?
A. Initial chest tube output of greater than 1,000 mL of blood
B. Initial chest tube output of greater than 10 mL/kg of blood
C. Persistent output of greater than 100 mL of blood per hour for the first 3 hours following chest tube placement
D. Persistent output of greater than 7 mL of blood per kilogram per hour following chest tube placement
Question 4
A 45-year-old woman with a history of hypertension and atrial fibrillation presents with a complaint of sudden onset vision loss in her right eye that occurred 10 minutes prior to arrival in the emergency department. She denies associated pain or trauma to the eye. Visual acuity is 20/20 at baseline, however she can now only count fingers on the right. What is the appropriate next step?
A. Arrange for 24-hour follow-up with ophthalmology
B. Digitally massage the globe
C. Obtain a CT scan of the head without contrast
D. Perform an anterior chamber paracentesis
Question 5

A 19-year-old man presents to the ED after jamming his finger while playing basketball. On exam, he has swelling and tenderness to the proximal interphalangeal joint and pain with proximal interphalangeal joint extension. An X-ray is negative for a fracture. To prevent the deformity seen in the above image from developing, what type of splint should be placed?
A. Distal interphalangeal joint in extension, proximal interphalangeal joint and metacarpal phalangeal joint with full range of motion
B. Distal interphalangeal joint, proximal interphalangeal joint, and metacarpal phalangeal joint in extension
C. Proximal interphalangeal joint in extension, distal interphalangeal joint and metacarpal phalangeal joint with full range of motion
D. Proximal interphalangeal joint in flexion, distal interphalangeal joint in extension, and metacarpal phalangeal joint with full range of motion
Question 6
Which of the following statements regarding anticonvulsant hypersensitivity syndrome is true?
A. Cross-reactivity between anticonvulsants is rare
B. Mucous membranes are spared early in the disease
C. Onset usually occurs after longstanding therapy
D. Rash is the most common initial symptom
- A Galeazzi fracture is a fracture of the middle to distal third of the radius with dislocation or subluxation of the distal radioulnar joint.
- In Galeazzi fractures, the anterior interosseous nerve (or AIN) is at risk. Check its function by testing the flexor pollicis longus and the flexor digitorum profundus by asking the patient to make an “OK” sign.
- Asking the patient to show you a “thumbs up” tests the radial nerve.
- The ulnar nerve is innervated by the C8–T1 spinal nerve roots.
- Hypomagnesemia can be seen in patients with chronic malnutrition, including alcoholics, children with restricted diets, and in the elderly. It is also seen in patients on diuretics, those taking aminoglycosides, and patients on a PPI. Concomitant hypokalemia is common.
- Hypomagnesemia typically presents with vague symptoms including muscle cramping and diffuse weakness. More serious complications include vertigo, ataxia, seizures, increased reflexes, and cardiac conduction abnormalities, such as atrial fibrillation, PVCs, and ventricular tachycardia.
- Indications for emergent thoracotomy in a patient with a traumatic hemothorax include:
- Initial chest tube drainage of over 20 ml/kg of blood
- >3 mL/kg/hr of blood for 4 hours
- Persistent bleeding of over 200 ml/hour for 3 hours
- Persistent bleeding of 7 ml/kg/hour
- Refractory shock
- Chest that remains more than half full of blood on chest X-ray despite tube insertion
- Traumatic hemothorax is usually due to lung parenchymal injury which is usually self-limited. It may also be due to small or large vessel vascular injury or even cardiac injury.
- Central retinal artery occlusion (CRAO) risk factors include hypertension, atrial fibrillation, diabetes, valvular heart disease, arteriosclerosis, hyperlipidemia, sickle cell anemia, carotid artery disease, and vasculitis.
- CRAO typically presents with acute painless vision loss followed by the development of a Marcus-Gunn pupil. On exam, you would expect a pale retina and cherry red macula.
- Treatment for CRAO includes digital globe massage and medications like acetazolamide, mannitol, topical timolol, and sublingual nitro. More advanced measures include hyperbaric oxygen and anterior chamber paracentesis.
- A boutonnière deformity, which has PIP flexion and DIP extension, is most commonly caused by rheumatoid arthritis, but may also be caused by trauma. In the traumatic setting, it is typically caused by a central slip injury.
- To treat presumed traumatic central slip injury, splint the patient in PIP extension, leaving the DIP and MCP in full ROM. If there is an associated fracture, internal surgical fixation may be required.
- Anticonvulsant hypersensitivity syndrome, now more broadly classified under DRESS, presents with a 1–2 week period of nonspecific symptoms followed by a diffuse erythematous rash. Severe cases are associated with fever, rash, and internal organ involvement and carry a 10% mortality.
- Treatment for DRESS is with IV steroids and immunoglobulin, in addition to supportive care and cessation of the offending agent.
So that wraps up Episode 21. Remember to follow us on Twitter @Roshcast and check out the new Teaching Image series on the blog.
Until next time,
Jeff and Nachi
Get Free Access and Join Thousands of Happy Learners

You must be logged in to post a comment.
Comments (0)