
Podcast Ep 43: Pulmonary Embolism, Colchicine & More




Always do your best. What you plant now, you will harvest later.
–Og Mandino
Welcome back to RoshCast for Episode 43! After a long pause, we are back with new episodes and a lot of announcements. A lot has happened in the past few months. Jeff had a baby and moved to Pittsburg to start his EMS fellowship. In doing so, he is taking a break from Roshcast to focus on fellowship and his new baby. Megha Rajpal, a fourth-year resident at Mount Sinai, will be taking over as co-host.

- For epiglottitis, the patient will usually have a rapid-onset fever and dysphagia. On exam, they could be leaning forward, drooling, and even have inspiratory stridor.
- The typical radiographic finding for epiglottitis is thumbprint sign, which is seen on a lateral neck film.
- The most common bacteria associated with epiglottitis are H. influenzae and Streptococcus.
- For management in epiglottitis, airway is the crucial piece. Patients may need to be intubated immediately. Don’t forget to start the patient on antibiotics to treat for the common pathogens.
Now onto this week’s podcast
Question 1
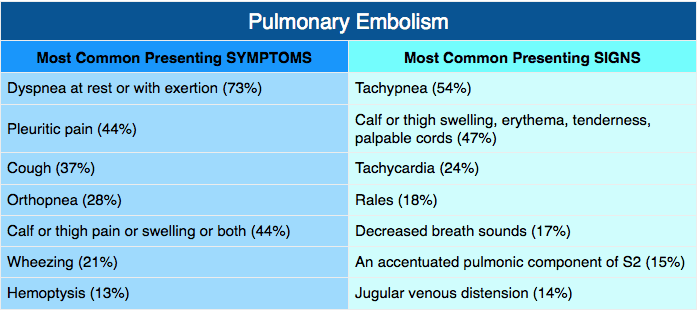
Which of the following is the most common presenting vital sign abnormality seen in patients presenting with a pulmonary embolism?
A. Fever
B. Hypoxia
C. Tachycardia
D. Tachypnea
Question 2
A 72-year-old man presents with pain in the right knee. It has increased over the last 24 hours with redness and swelling. Joint aspiration reveals negative birefringent crystals. He reports an allergy to NSAIDs and is a brittle diabetic. Colchicine is prescribed. Which side effect limits its usefulness due to a narrow therapeutic window?
A. Headache
B. Nausea and vomiting
C. Rash
D. Sore throat
Question 3
A patient presents to the ED after waking up and finding that he was drooling while drinking his coffee. When he looked in the mirror he noticed that the left side of his face was drooping. Which of the following findings is suggestive of a central process?
A. Hyperacusis of the left ear
B. Inability to close the left eye completely
C. Loss of taste sensation
D. Preserved ability to raise the eyebrows
Question 4
Which of the following is considered a stable cervical spine injury?
A. Bilateral facet dislocation
B. Clay-shoveler’s fracture
C. Hangman fracture
D. Teardrop fracture
Question 5
A 28-year-old man presents to the emergency department via ambulance after a terrorist set off a large bomb in an airport. On physical exam, he has bilateral tympanic membrane ruptures. Chest X-ray shows bilateral pulmonary contusion. These injuries are most consistent with which category of blast injury?
A. Primary
B. Quaternary
C. Secondary
D. Tertiary
Question 6
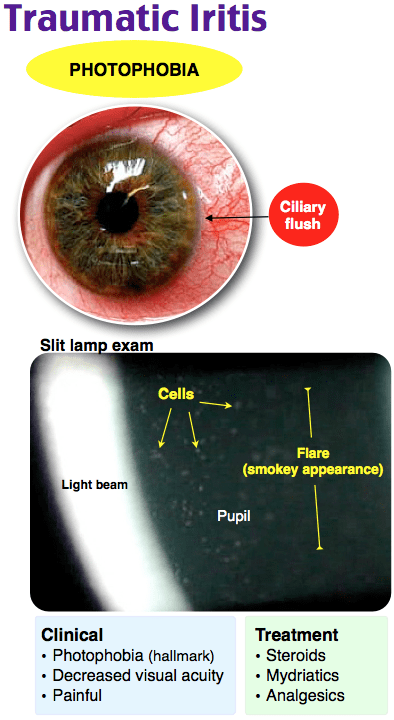
A 19-year-old man presents with eye pain and photophobia in his left eye after being punched there two days ago. He describes blurry vision. On exam, you note consensual photophobia. Which of the following is the most appropriate treatment?
A. Homatropine drops
B. Timolol
C. Topical ketorolac drops
D. Topical vasoconstrictor
- Tachypnea is the most common presenting vital sign abnormality for a pulmonary embolism, while dyspnea at rest or exertion is the most common presenting symptom.
- Joint aspiration in gout demonstrates negative birefringent monosodium urate crystals. NSAIDs are the first-line treatment.
- Colchicine can cause severe GI symptoms in more than 10% of patients.
- When deciding on a central versus peripheral etiology for facial paralysis, preserved ability to raise the ipsilateral eyebrow or close the ipsilateral eye is more concerning for a central lesion than a peripheral lesion.
- Clay shoveler’s fracture is a stable avulsion fracture of the spinous process of C6–C7.
- Jefferson burst fracture, bilateral facet dislocation, odontoid type II and type III fractures, any fracture with a dislocation, hangman’s fracture, and teardrop fracture are all unstable cervical spine fractures.
- Primary blast injury occurs from direct effect from blast shockwaves.
- Secondary blast injury occurs from the impact of fragments due to exploding devices.
- Tertiary blast injury occurs when the blast wave propels the body into objects.
- Quaternary blast injury is due to environmental contamination from the device.
- In quinary blast injuries, there is bodily absorption of device additives.
- Traumatic iritis is treated using cycloplegics like homatropine and topical steroids.
That wraps up RoshCast Episode 43! Rosh Review is excited to announce the launch of a new podcast called The PA Way hosted by Alison Callahan, PA-C. Definitely worth a listen. Be sure to also check out the RoshCast blog for questions from this episode and prior episodes, related images and tables, as well as bonus teaching points. There are also tons of other great free resources there to help prepare you for the boards and the wards.
Don’t forget to follow us on twitter @RoshCast and @RoshReview. And you can always email us at RoshCast@RoshReview.com with any feedback, corrections, or suggestions. You can also help us pick questions by identifying ones you would like us to review. Write “RoshCast” in the submit feedback box as you go through the question bank. Lastly, if you have a minute, make sure to rate us and leave comments on iTunes to help spread the word about RoshCast.
Megha and Nachi
Get Free Access and Join Thousands of Happy Learners

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
You must be logged in to post a comment.
Comments (0)